
The conversation about pain bias in health care and the dismissal of women and the marginalized queer-trans community’s symptoms has been ongoing for decades. Science and evidence have emerged to show how sex and gender impact various diseases, yet our healthcare delivery model lags. Some medical practitioners still practice medicine based on the problematic “one-size-fits all” approach to diagnosis and treatment. A sex- and gender-based approach to disease management is not even on their radar.
Female hysteria was once a common medical diagnosis for women, applied whenever women displayed “inappropriate” emotions such as anxiety, anger, and even sexual desire. There’s this pervasive belief in the medical community, that every time a woman or gender-nonconforming individual complains about health, it is either related to hormones or all in the head. For women, how often she gets angry, only to be asked if she’s about to get her period? Or how often she complains about weight gain, only to be told that it’s related to hormones. It isn’t the hormones making them anxious or upset but the condescending attitudes.
For centuries, it was believed that the uterus itself was the cause of a woman’s “hysterical” symptoms as the word “hysteria” is derived from the Greek word “hysteria” which means uterus. Even Hippocrates believed that the womb traveled throughout the body causing hysteria, a psychological diagnosis that was only removed with the updated Diagnostic and Statistical Manual of Mental Disorders, 3rd ed, in 1980.
Within cisnormative social and cultural structures, there is a large amount of hate speech, exclusion, and trickery, as well as institutional, structural, cultural, and interpersonal dominance, and control against the trans and gender-diverse community using the tool of gaslighting. Several recent studies have highlighted that transgender people experience high levels of identity-related abuse. Identity-related abuse can involve physical, emotional, and/or financial abuse concerning gender and gender presentation. More specifically, this may involve denying someone is transgender, commenting negatively about a person’s appearance or body, or intentionally using the wrong pronoun and/or name. Asking someone to not disclose they are transgender to others, threatening to tell other people that someone is transgender, and withholding medicine or money for medicines or surgery in the medical setting invalidates their mere existence.
Also Read: The History Of ‘Hysteria’ And How Science Can Be Sexist
The HIV/AIDS intervention approach led to a lasting wrongful portrayal of queer-trans individuals as solely being held responsible for the epidemic. There hasn’t been a conversation regarding the health of people with a compromised immune system, queer-trans-friendly mental healthcare, queer/trans friendly staff, and caretakers. Queer/trans people, who are already discriminated against, are still socially seen as disease-carrying individuals to be avoided and isolated at all costs. They are 49 times more likely to be HIV infected than the general population (Baral et al 2013). In India, the estimated queer/trans-HIV prevalence (9%) is 20 times that of the cis-population, the highest being among sex workers (NACO 2014a).
Gaslighting can be differentiated from other forms of bullying in medicine because it does not involve public humiliation, specific threats, or blatant insults. It is more subtle and private. While it might not result in full-blown delusions or misshaping of memory, this abuse can have lasting effects on the self-esteem and mental health of the people seeking help.
Gaslighting is entrenched in power structures. Women often lack the cultural, economic, and social capital to effectively gaslight men, hence patriarchal power structures are exacerbated by intersecting issues of age, social class, race, and gender.

Research suggests that diagnostic errors occur in one out of every seven encounters between a doctor and patient, most of these mistakes driven by the physician’s lack of knowledge. India has encountered several experimental practices of gender-transforming procedures. Patients have been gaslighted into doing so, without being consulted about the process.
For the most part, doctors aren’t intentionally dismissive. Doctors often work under immense pressure and are overburdened. With only so much time to allot to each patient in a day, oversight is easy and mistakes do happen. They get so deep into pure facts and figures that they tend to forget the human aspect of it. They stop paying attention to what each individual is saying and mentally start running through the disease checklist they have memorized all the years. A doctor’s visit or getting medical attention is a collaborative experience, and one deserves to feel listened to. If the provider is being dismissive, one needs to push back to come up with a diagnosis and treatment plan together, else finding another doctor is suggested.
Also Read: How Has Science Aided In The Oppression Of Gender Minorities?
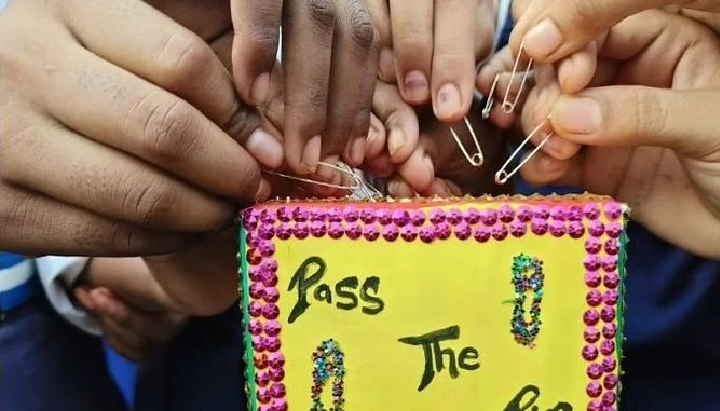
Women in Bihar initiated a campaign “pass the safety pin” to raise a call for dignified healthcare and voice a collective demand to create safe spaces where they can seek treatment without judgment. They shared their stories of gendered discrimination while accessing medical care. The safety pin was chosen because of its accessibility for women from all walks of life.
World-famous tennis champion Serena Williams has dealt with medical gaslighting that nearly cost her her life. In a Vogue interview, Williams opened up about her medical complications post-delivery. With a history of pulmonary embolisms, she knew something was wrong. It took insisting on convincing on her part to get the medical team to take her seriously.
Another case had been reported against the SNR Carnival hospital, Kalyani. The institution supposedly performed a hysterectomy on a woman in 2013, even though there was no direct indication of malignancy in the uterus or ovary of the patient who then suffered post-hysterectomy Vesicovaginal Fistula (VVF). Eventually, the patient underwent a further operation at CMC, Vellore that incurred huge expenditure. The council claimed that the couple was not suggested alternative methods, and the procedure was performed without informed consent, which violates the principle framed by the Medical Council Of India and other organizations. The case is being actively reviewed and a decision will be made accordingly.
Also Read: Fake Narratives By Pseudo-Patriarchal Science For Bodies Of All Women
Several cases have been recorded where patients especially women and the minority community who already struggle to access medical facilities have not been taken seriously when they shared their painful experiences. They are more likely to receive sedatives rather than the pain medication they need.

Obstetric violence – abusing pregnant women is common in Indian Medical System and hardly discussed. There have been records during childbirth, where women were mistreated and did not feel heard. Due to the social norm stating women as child bearers can endure pain with ease, the medical practitioners denied mothers’ reality. They are expected to feel the pain and not complain, or else they face abuse.
One such case happened in Keonjhar, Orissa. A pregnant lady died due to negligence and poor treatment by the District Headquarters Hospital, Keonjhar on 23 March 2016 while undergoing a cesarean operation. According to the reports, her expected date of delivery was 23 March 2016. On 22 March 2016 she felt labor pain and was immediately rushed to the hospital, but was sent back home as the doctor in charge of examining her claimed it was a false pain. She had to be admitted to the hospital again within a few hours due to severe pain. Eventually, after delivering her infant, she passed away because of the mere negligence of the authority and the medical staff. Although they compensated the family, we cannot overlook the lost life. Unfortunately, cases like this occur too often.
Also Read: How Psychology Wronged Women
When it comes to the people from the marginalized community – the queer-trans, parents, and doctors act in what they believe is in the best interest of the child. They operate on the infant to conform the body to the “normal” male or female. For instance, a baby with dominantly female characteristics and a clitoris larger than ‘normal‘ could appear like a small penis. Parents go for surgery to cut the clitoris to the normal size. This amounts to female genital mutilation, a grievous human rights violation.
Sometimes in dignifying the “social norm” too much, we lose a lot along the way.
Manisha (she/her) is the Junior Social Media and Content Manager at Rangeen Khidki Foundation. She is a student pursuing Master’s in Computer Science and takes deep interest in SRHR and research.
Rangeen Khidki Foundation is a feminist youth led organisation based in Kolkata working in the space of sexual and reproductive health and rights.
You can find them on their Website, Instagram, Facebook and LinkedIn.


