As the government celebrates the new, improved vaccine policy that started in the country on June 21, promising free vaccines to all, along with much needed on-spot registrations, there is much left to be done. Weeks away from the projected third wave of the pandemic, the state must vaccinate the people, not only quickly, but strategically.
It is no secret that the pandemic has pushed women’s freedom back by ages, solidifying gender roles within families, depriving women of essential access to public space, resulting in women students dropping out of schools and colleges, facing abuse within the closed spaces of the home, and bearing the violence of inequality and oppression.
Also read: Poster Series: Covid-19 Vaccine And Class-Caste Divide
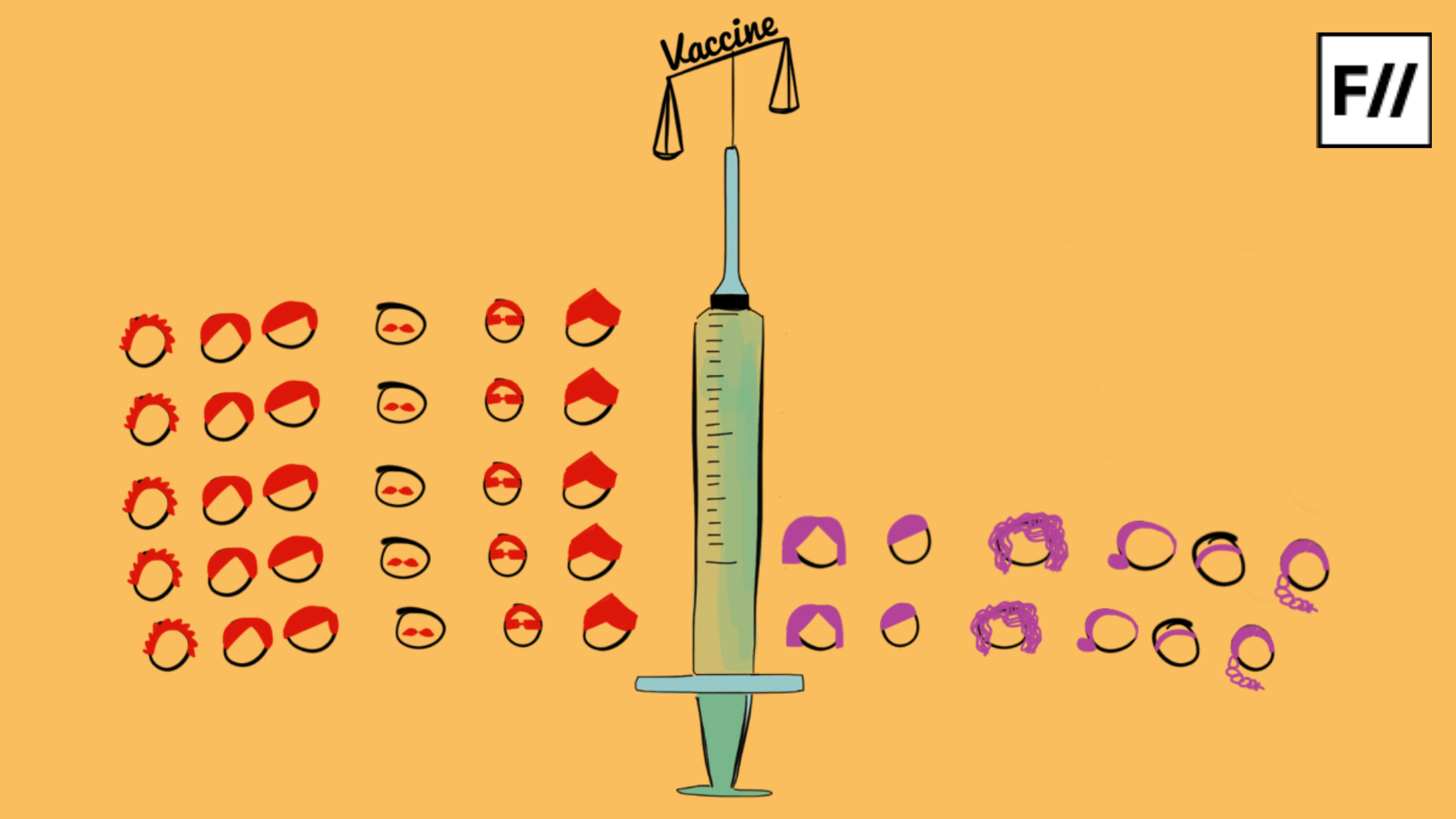
As the country makes efforts to protect its citizens, we see yet again that women have been left behind. As of June 21, India has registered 27.4 crore vaccine doses – only about 3.6% of the population has been vaccinated. Of these, an overwhelming amount is men – women are getting left behind. There is a very clear gender gap being seen in vaccinated people. For about 1000 men, only 725 women are being vaccinated in Delhi. Nationally, the ratio is still a dreadful 1000:857.

As of June 21, India has registered 27.4 crore vaccine doses – only about 3.6% of the population has been vaccinated. Of these, an overwhelming amount is men – women are getting left behind.
What are we doing wrong? It is easy to roll out policies, easier to praise them. But are we taking into account structural inequalities that are preventing people from accessing these? Studies have shown that women are more vulnerable to fatal consequences after contacting the virus. Women workers are coming into contact with the virus at all times – especially in the unorganised sector. They are engaging constantly in caring for the sick inside homes. This warrants special attention. The task at hand is not just to vaccinate, but to vaccinate everyone, making sure that protection goes right down to the most vulnerable.
An understanding of gender and how it permeates our society is necessary to achieve this objective. The most visible problem would be that of the digital divide. A huge number of women do not own smartphones. Besides, the ability to use technology and access the internet is often controlled by families. In such circumstances, it is wrongful to expect them to schedule appointments to get vaccinated.

The problem being the digital divide suggests that gender disparity in vaccinations might be a rural-only issue. But ‘progressive’ urban areas are no better off. Statistics from South Delhi show that a whopping 53% more men are getting vaccinated, compared to women. In Mumbai too, men are 23% more in number. To suggest that digital illiteracy and lack of access to the internet is the only problem would be to turn a blind eye to the entrenched gender inequality in our private spaces.
Gender norms and power structures in the family inevitably affect access to healthcare for women. In most communities, women do not enjoy much mobility. Dependence on men for travel, even for the shortest distances, directly hinders their ability to access hospitals or vaccination centers to get their shots.
Also read: CoWIN App & The Survival Of The Fittest (And Fastest) In The Vaccination Drive
But vaccine inequality is not just the story of COVID-19. The gender gap persists in all cases, it existed well before COVID-19 was ever a thing, and will continue to exist. In urban areas in India, girl children are 22% less likely to get a full course of vaccination than their male counterparts. Like in most things, parents are choosing to get sons vaccinated before girls – trying to save on time and money. It is interesting to note that South Asian countries are the only countries where female infants have a lesser chance of survival up to their first birthday, compared to other countries where this is the case for male children, owing to natural, biological differences. This is only due to differential treatment that deprives girl children of nutrition, healthcare and nourishment.
The question dials down to agency: are women empowered enough to choose to get vaccinated themselves, visit vaccination centers without dependence on men, and access healthcare proportionately whenever the need arises? Increased autonomy for women within families and communities will not only translate to being able to get vaccinated themselves, but also to help younger women and children get vaccinated when the time comes. When women get a say in decision making, get control over collective resources and obtain increased mobility, only then will we able to achieve a semblance of equitability in healthcare and immunisation.
Women have been historically disadvantaged in epidemic situations. More women have died than men in most widespread epidemics, and the same circumstances prevail that would have prevailed a hundred years ago that created such disadvantage. The Zika virus in Brazil, for example, impacted women more than men, due to lack of access to clean water, sanitation, healthcare and information.
The situation is even worse for gender minorities. As of 17 May, only about 20,269 trans people were vaccinated. On June 2, the number was only a little larger – 26,793. The lack of data is not helping anyone. There is little data to show the caste and class disparity that has surely intersected with the gender gap in immunisation. Questions of healthcare and vaccination cannot be divorced from broader struggles of equality, fairness, justice and responsibility, and moving forward, taking structural inequalities into account is imperative.
There is no one solution to the problem, but there is the need to center women and other gender minorities in the fight against COVID-19. Planning must not just include women in its ambit, but women should be actively involved in it.
There is no one solution to the problem, but there is the need to center women and other gender minorities in the fight against COVID-19. Planning must not just include women in its ambit, but women should be actively involved in it. The idea is to have a community approach, mobilising women and listening to them, being vigilant of gender dynamics and working around them. Ensuring safe and inclusive spaces for women to discuss grievances and work together towards ensuring for themselves health and protection is the way to go.
The impact of the pandemic has not been gender neutral, and the fight against it cannot either. Placing gender at the center of COVID-19 recovery efforts is necessary and undeniable. There is much to be rebuilt, much to be restored, and the most vulnerable must not be pushed deeper into spaces of oppression.
Stuti Srivastava is an undergrad student of Political Science at the University of Delhi. She likes to explore issues at the intersection of gender, policy and society. You can find her on Instagram.
Featured image source: Ritika Banerjee/Feminism In India